My Two Pelvises
Often clients come in with a very specific pain in their sacral base (the juncture between L 5 and the top of the sacrum). It’s usually very much in the center and often constant although slightly worse when bending forward. I can usually tell what is going on based on the pantomime they use to show me where it hurts. The visual description I get referring to this annoying type of pain usually points fingers to what is known as Flexion Disorder.
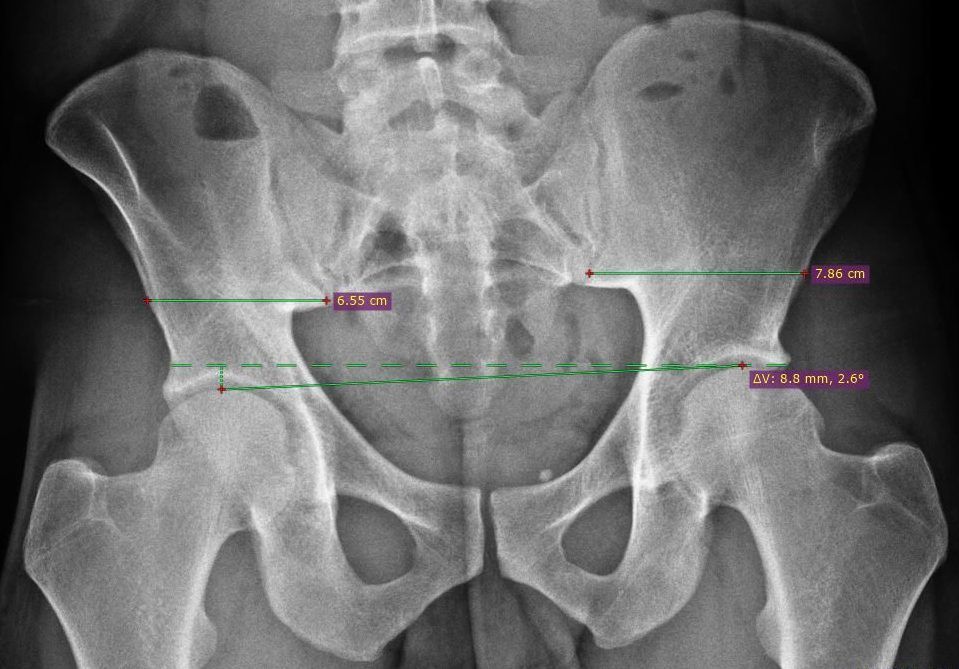
We often think of the pelvis as one block of bone that has various places you could point to and call a “hip” but it’s interesting to discover that the adult pelvis has two halves with a wedge between the two in the back called the sacrum; so three parts in total. The pubic bone is not one bone at all but rather the coming together of these two halves with a cushion of cartilage between the two called the pubic symphysis.
The two pelvic halves, called the innominate bones, have very different personalities. One may be shy like a dog with his tail between his legs, while the other may be very outgoing and almost promiscuous as if implying a sexual invitation. Likewise, one may want to swing out like a wide open swinging door, while the other may want its door merely cracked slightly open. The obturator foramen, or holes at the bottom of the pelvis, may look like one is wearing cat eye glasses while the other is simultaneously wearing John Lennon glasses! Silly multi personality pelvis.
These differences can wreak havoc on the low back. All the different angles, directions, and facings put a torque force on the place where the spine ends and the sacrum begins. The question is: what’s controlling the placement of these two fraternal twin halves of the pelvis?
The answer is a question: What came first the chicken or the egg? One could argue that it is coming from the spine where the concave or convex part of a lateral curve can give distinct direction to the placement of the pelvis respectively. Another would argue that it’s all in the head… the placement of the temporal bones or the sub occipitals, or even the neck – like an “as above so below” scenario. I want to keep it fairly simple and peer into how the legs can have a huge influence on the two innominate halves of the pelvis.
Think of the how strong human legs naturally are. They were made for us to run and climb and walk for miles on end. Imagine the strength of the thighs in the back, or hamstrings tugging the pelvis down at the attachments on the sits bones. This action creates a pelvic tuck situation – one that you may use in a Pilates “imprint” or a yoga “cat” pelvis. Now imagine what tight hip flexors can do as if tugging the hip points, or ASIS, down from the front as if sticking out the buttocks, or a yoga “cow” situation. What if one side is doing “cat” and the other side is doing “cow” and the body is stuck like that wether you’re sitting, standing, or walking.? That is exactly what is going on during a flexion disorder of the pelvis. Two personalities, two different stories, one body.
Why this happens can be usually traced back to movement patterns stemming from trauma or habits, and/or spinal propensity based on scoliotic curves. What’s important here is just to keep the pelvis balanced. Understanding the disparity is the key to knowing what to do. A typical flexion disorder causing a lot of pain at the base of the spine could be helped by simply foam rolling your quad on one side and stretching your hamstring on the other. Get measured by a knowledgeable therapist and you can help yourself even at home on your own! Awareness is key and knowledge is power.
By Shila Tirabassi LaGrua
The post My Two Pelvises appeared first on Body Center St. Pete.